History of Present Illness
42-year-old male brought in by EMS. Jumped onto the T (subway) tracks to rescue a woman who had fallen. After successfully pulling her off the tracks, he slipped while climbing back up the platform, fell backward, and struck his head. EMS noted agonal respirations. They were unable to intubate in the field and placed an LMA (Laryngeal Mask Airway) prior to transport.

Emergency Department Course
Triage & Initial Resuscitation
Trauma arrival directly from EMS.
+1
Triage & Initial Resuscitation
Trauma arrival directly from EMS.
Medical Decision Making
Patient has agonal respirations and a GCS of 5, requiring immediate definitive airway control. However, there is excessive bleeding in the oropharynx. Combined with the finding of atrial fibrillation on the monitor, there is a high clinical suspicion that the patient is therapeutically anticoagulated (e.g., on a DOAC). Must prepare for rapid sequence intubation (RSI) and simultaneous pharmacological reversal in case of an intracranial hemorrhage.
Diagnostics & Findings
- E-FAST (Extended Focused Assessment with Sonography for Trauma)
Findings:
- Good breath sounds bilaterally.
- Pupils 4mm and reactive.
- Excessive oropharyngeal bleeding noted.
- Atrial fibrillation observed on cardiac monitor.
Interventions
- Ordered RSI medications: 120mg Ketamine, 80mg Rocuronium.
- Instructed team to stand by with 4-factor Prothrombin Complex Concentrate (PCC).
- Instructed staff to search for medical records regarding DOAC use.
⮑ Outcome & Reassessment
Patient prepared for definitive intubation. Hemodynamics tolerate initial assessment.
Clinical Media

Airway Management & Neuroprotection
Need for definitive airway and neuroprotection prior to imaging.
+2
Airway Management & Neuroprotection
Need for definitive airway and neuroprotection prior to imaging.
Medical Decision Making
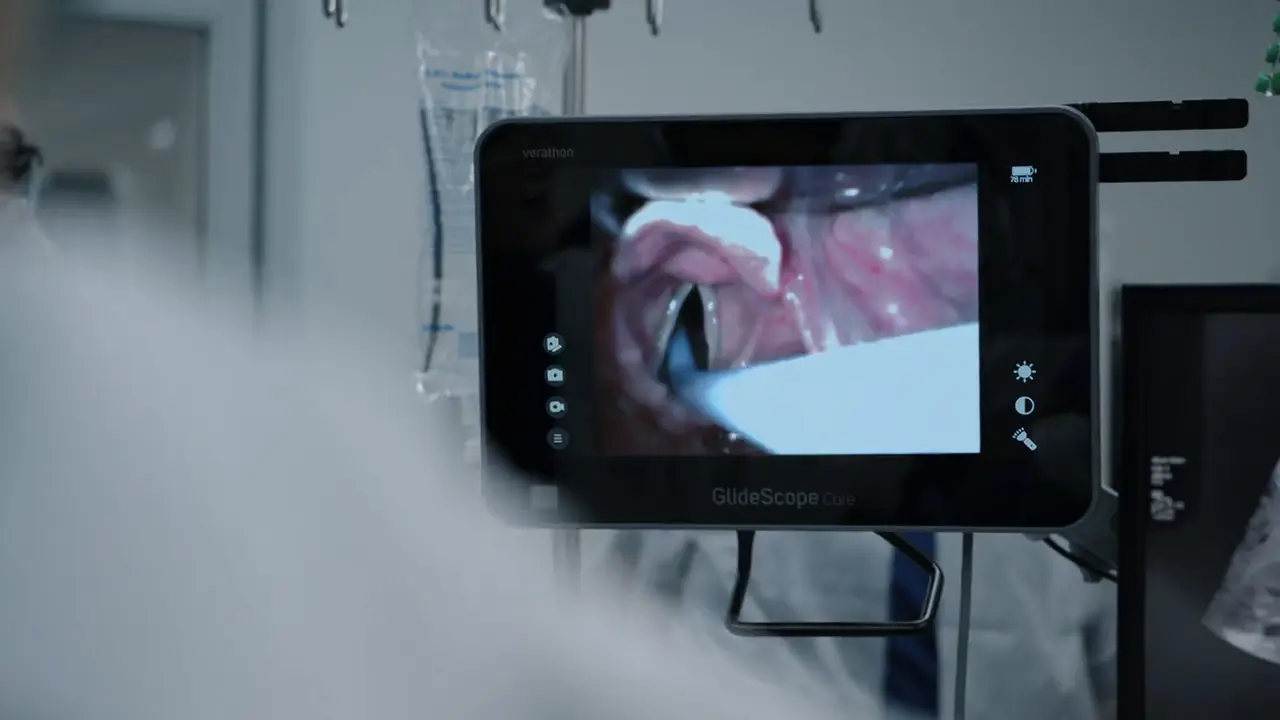
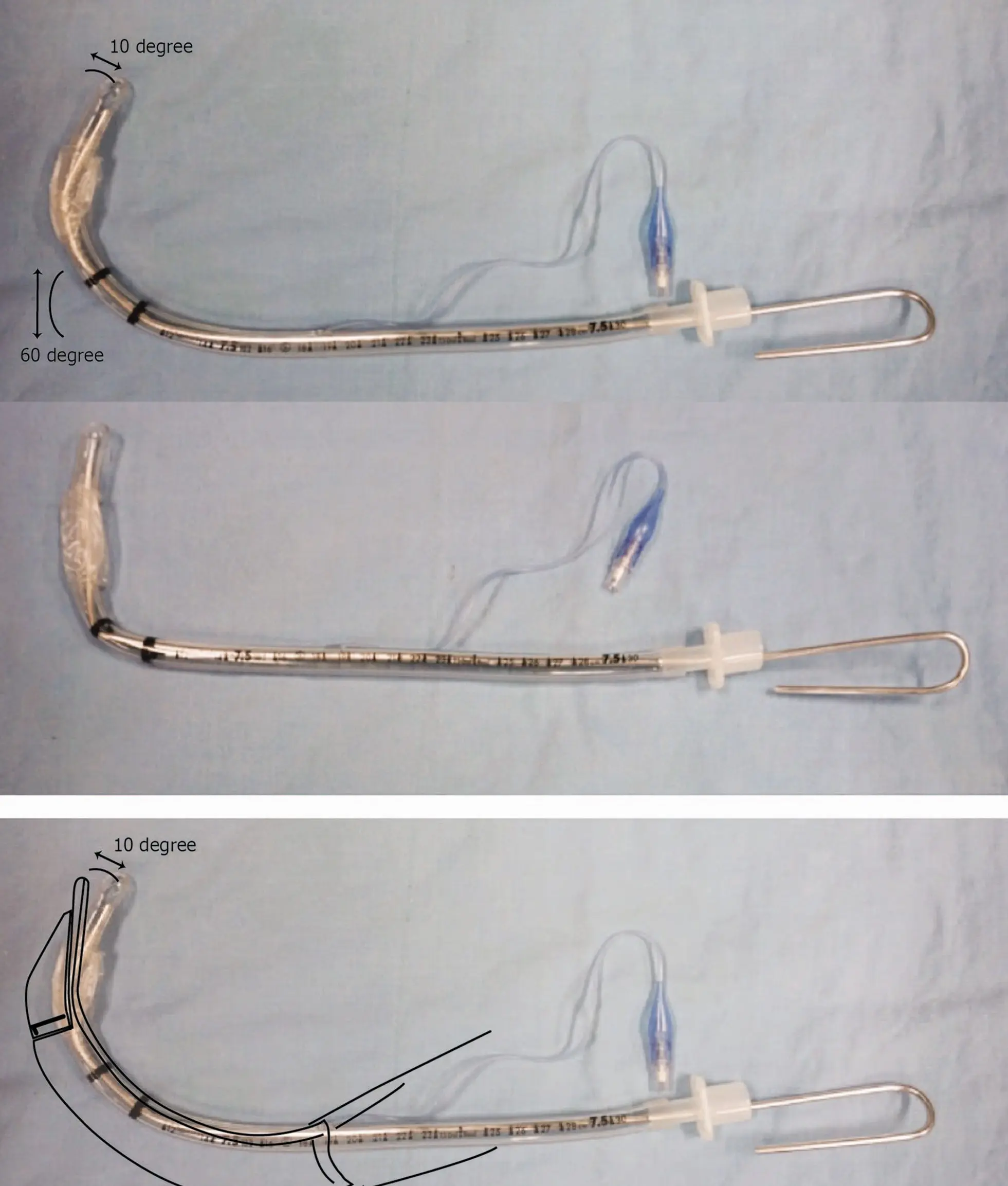
Cervical spine immobilization prevents neck flexion/extension, making the vocal cords appear very anterior. A rigid stylet bent into a 'hockey stick' shape is required inside the endotracheal tube to navigate the difficult airway. Due to high suspicion of intracranial bleed on blood thinners, empiric administration of 4-factor PCC (clotting factors II, VII, IX, and X) is superior to FFP due to speed of reconstitution and lower volume. Mannitol is added to decrease intracranial pressure via osmotic diuresis before the patient goes to the CT scanner.
Diagnostics & Findings
Findings:
- Anterior vocal cords due to C-spine precautions preventing neck flexion.
Interventions
- Endotracheal intubation utilizing an endotracheal tube with a 'hockey stick' bent stylet.
- Administered 4-factor PCC.
- Administered 80g Mannitol.
- Patient transported to Head CT.
⮑ Outcome & Reassessment
Airway successfully secured. Patient stabilized enough for transport to radiology.
Clinical Media
Imaging Review & Disposition
Head CT results returning from radiology.
Imaging Review & Disposition
Head CT results returning from radiology.
Medical Decision Making
The CT scan reveals a small left temporal intraparenchymal bleed, but lacks an epidural or subdural hematoma, and crucially, lacks midline shift. This indicates the primary injury is relatively small and the Mannitol/PCC interventions may have prevented catastrophic expansion. He requires close neuro-monitoring in the ICU, prophylactic antiepileptics to prevent post-traumatic seizures which could increase ICP, and serial imaging to ensure the bleed remains stable.
Diagnostics & Findings
- Non-contrast Head CT
Findings:
- Small left temporal intraparenchymal bleed.
- No epidural hematoma.
- No subdural hematoma.
- No midline shift.
Interventions
- Keppra (Levetiracetam) loading dose ordered for seizure prophylaxis.
- Scheduled repeat Head CT in 3 hours (or immediately if pupillary changes occur).
- Consulted intensive care for ICU admission.
⮑ Outcome & Reassessment
Patient remains critically ill with an uncertain neurological prognosis ('maybe he wakes up, maybe not'), but brain anatomy is currently stable.
Diagnoses & Disposition
Evolving Diagnoses
- [00:10:56]Severe Traumatic Brain Injury (GCS 5)
- [00:10:56]Atrial Fibrillation with suspected systemic anticoagulation
- [00:16:55]Left Temporal Intraparenchymal Hemorrhage
Current Disposition
Intubated, stabilized, and boarding in the ED while waiting for an available ICU bed. Plan for repeat Head CT in 3 hours.
Casebook Analysis
Episode Context
Sam Wallace serves as the high-acuity, emotionally resonant trauma case for the pilot episode. As a 'Good Samaritan' who risked his life for a stranger only to suffer a devastating brain injury, his narrative underscores the unpredictable and often tragic nature of emergency medicine. His case also highlights the systemic issue of ED boarding, as he must wait in the emergency department for an ICU bed.
Attending's Review
Medical Accuracy
The medical management depicted is highly accurate and represents excellent emergency care. Deducing that a trauma patient in Atrial Fibrillation with unexpected oral bleeding is likely on a DOAC is a great clinical catch. The decision to empirically administer 4-factor PCC (which contains factors II, VII, IX, and X) and Mannitol prior to CT scanning is an aggressive but realistic protocol for a rapidly declining trauma patient suspected of an expanding intracranial bleed. Furthermore, the intubation dialogue ('cords are very anterior... keep the hockey stick straight up') perfectly describes the technique of shaping a rigid stylet inside an endotracheal tube into a 'hockey stick' bend to navigate a difficult airway complicated by cervical spine precautions.
Complications & Errors
- No direct medical errors made by the staff; however, the case was complicated pre-hospital by EMS inability to secure the airway, leading to an LMA placement.
- Oropharyngeal bleeding secondary to likely anticoagulant use complicated visualization of the vocal cords during intubation.
Clinical Pearls
In trauma patients presenting with an irregular heartbeat (Atrial Fibrillation), maintain a high index of suspicion for systemic anticoagulation, which drastically increases the risk of catastrophic intracranial hemorrhage.
When securing an airway in a trauma patient with a suspected C-spine injury, the traditional 'sniffing position' cannot be used. Advanced adjuncts like a rigid stylet bent into a 'hockey stick' shape or a bougie with a coudé tip are essential for navigating anterior airways.
4-factor Prothrombin Complex Concentrate (PCC) provides rapid, low-volume reversal of Vitamin K antagonists and certain Direct Oral Anticoagulants (DOACs), making it a crucial intervention in life-threatening bleeds prior to imaging confirmation.