History of Present Illness
A 31-year-old healthy male presents with shortness of breath and severe fatigue. He reports feeling fine until about two weeks ago, following the Rochester Marathon. He frequently participates in triathlons. Attempted to run this morning but had to quit after one minute due to dyspnea. No recent falls, injuries, or previous medical issues reported.

Emergency Department Course
Initial Evaluation & First Cardiac Arrest
Patient suddenly loses consciousness and pulse while blood is being drawn.
+1
Initial Evaluation & First Cardiac Arrest
Patient suddenly loses consciousness and pulse while blood is being drawn.
Medical Decision Making
Patient went into pulseless ventricular tachycardia. Given his age and fitness, an acute MI is less likely but possible. Immediate defibrillation is required to restore perfusing rhythm.
Diagnostics & Findings
- Quick look with defibrillator paddles
- Blood draw initiated (Red and Purple top tubes)
Findings:
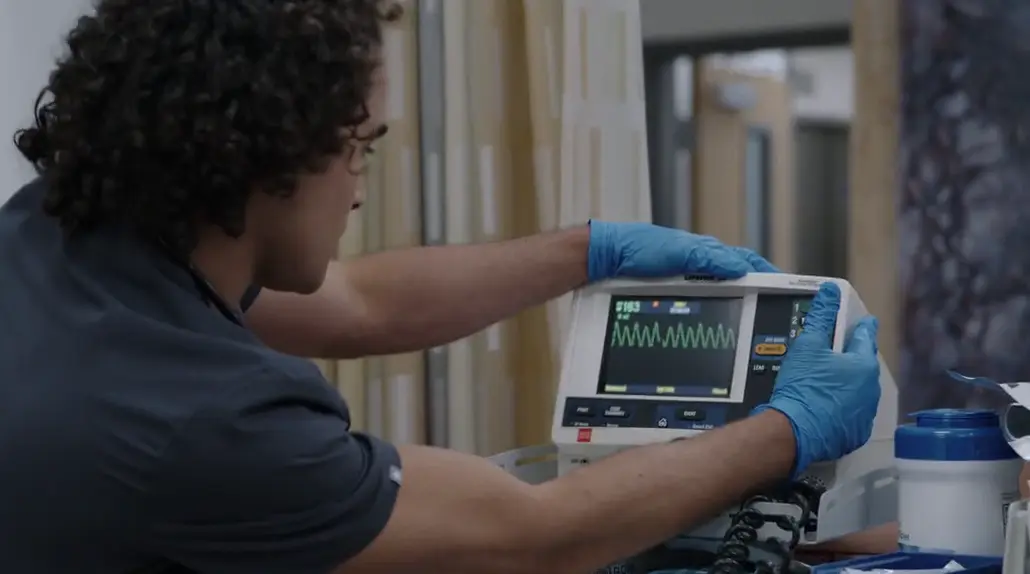
- Ventricular Tachycardia (V-Tach) on monitor
Interventions
- Sublingual Nitroglycerin (given prior to arrest)
- Defibrillation at 200 Joules
⮑ Outcome & Reassessment
Returned to Normal Sinus Rhythm (NSR) with one shock. Patient regained consciousness.
Clinical Media
Second Cardiac Arrest & Empiric Treatment
Patient groans and returns to V-Tach on the monitor shortly after first resuscitation.
Second Cardiac Arrest & Empiric Treatment
Patient groans and returns to V-Tach on the monitor shortly after first resuscitation.
Medical Decision Making
Recurrent V-Tach. Monitor shows widened QRS and peaked T-waves post-shock, which are hallmark signs of severe hyperkalemia. Given the history of extreme exercise, the patient likely has rhabdomyolysis causing acute renal failure and potassium retention. Immediate cardiac membrane stabilization with calcium gluconate is required before lab confirmation, overriding peer concerns about hypercalcemia.
Diagnostics & Findings
- Continuous EKG monitoring
- i-STAT point-of-care labs (pending)
Findings:
- Recurrent Ventricular Tachycardia
- Widened QRS and peaked T-waves on EKG post-shock
Interventions
- Defibrillation at 200 Joules
- 5L Nasal O2
- 1 gram Calcium Gluconate IV push (empiric)
⮑ Outcome & Reassessment
Returned to sinus rhythm after shock. QRS narrowed immediately after Calcium Gluconate administration. Patient stabilized temporarily.
Lab Confirmation & Medical Management
Point-of-care labs return confirming the suspected metabolic derangement.
Lab Confirmation & Medical Management
Point-of-care labs return confirming the suspected metabolic derangement.
Medical Decision Making
Labs confirm life-threatening hyperkalemia and acute renal failure. Calcium gluconate stabilized the myocardium, but the potassium must be shifted intracellularly immediately using insulin and glucose. The definitive treatment for this level of renal failure and hyperkalemia is hemodialysis. A central line (Quinton catheter) must be placed to facilitate this.
Diagnostics & Findings
- i-STAT blood analysis review
Findings:
- Potassium 7.7 mEq/L
- Creatinine 5.6 mg/dL
Interventions
- 10 units Regular Insulin IV
- 25 grams Glucose IV
- Preparation for ultrasound-guided Femoral Quinton catheter placement
- Consulted Renal for emergent hemodialysis
⮑ Outcome & Reassessment
Medications administered to bridge patient until hemodialysis machine and tech arrive.
Bedside Patient Education
Patient is alert and asks why his heart was shocked.
Bedside Patient Education
Patient is alert and asks why his heart was shocked.
Medical Decision Making
Patient requires counseling on his condition to understand the severity of overexertion without proper hydration, ensuring compliance with upcoming dialysis and future preventative measures.
Diagnostics & Findings
Interventions
- Patient education regarding muscle breakdown (myoglobin) damaging kidneys
- Explanation of potassium buildup causing electrical heart issues
- Counseling on the necessity of dialysis to clear potassium and allow kidney recovery (1-2 weeks)
⮑ Outcome & Reassessment
Patient understands the correlation between his triathlon training, dehydration, and cardiac arrest. Agrees to hydrate properly in the future.
Clinical Status Update
Routine follow-up on critical boarders in the ED.
Clinical Status Update
Routine follow-up on critical boarders in the ED.
Medical Decision Making
Insulin/Glucose and Calcium therapies are acting as a successful bridge. Definitive care is pending arrival of resources.
Diagnostics & Findings
- Repeat Potassium check
Findings:
- Potassium decreased to 6.1 mEq/L
Interventions
- Dialysis order confirmed written by Renal
- Awaiting dialysis tech arrival (estimated 15 minutes)
⮑ Outcome & Reassessment
Medical management successfully temporized the hyperkalemia. Patient remains stable pending definitive dialysis.
Hemodynamic Collapse & Emergent Procedure
Patient's blood pressure crashes while awaiting dialysis tech.
+1
Hemodynamic Collapse & Emergent Procedure
Patient's blood pressure crashes while awaiting dialysis tech.
Medical Decision Making
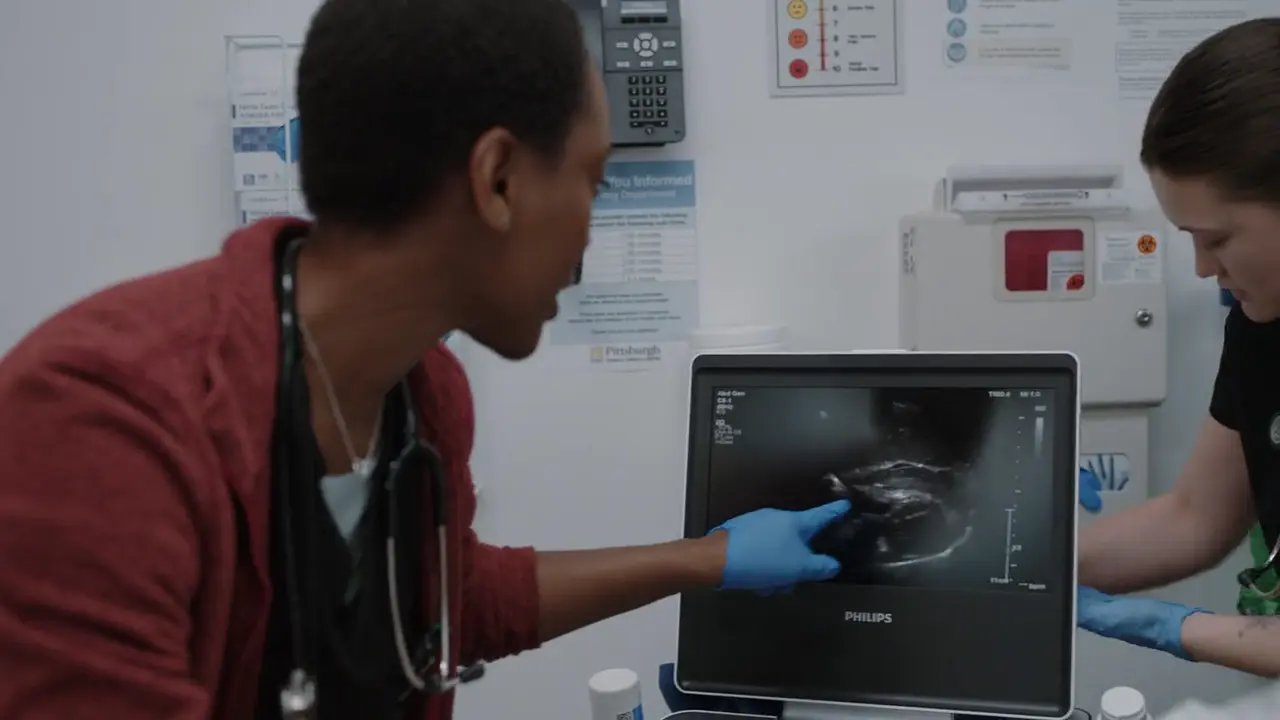
Acute severe hypotension in the setting of acute renal failure (uremia). Bedside ultrasound confirms a uremic pericardial effusion causing diastolic collapse of the right atrium and right ventricle, establishing the diagnosis of cardiac tamponade. The heart cannot fill properly. Emergent pericardiocentesis is required immediately to relieve the external pressure on the heart before full arrest.
Diagnostics & Findings
- Point-of-care Ultrasound (POCUS) / Echocardiography
Findings:
- Diastolic collapse of the right atrium and right ventricle
- Large pericardial effusion
Interventions
- 15 liters O2 via non-rebreather
- 25 mg Propofol IV
- 10 cc Lidocaine with Epinephrine (local anesthesia)
- Ultrasound-guided Pericardiocentesis (subxiphoid approach using 18-gauge thin wall needle)
- Aspiration of 3 cc pericardial fluid
- Placement of guide wire and triple lumen catheter
⮑ Outcome & Reassessment
Aspiration of a small amount of fluid successfully relieved the tamponade physiology. Pulse ox improved to 99%, BP normalized to 124/78.
Clinical Media
Diagnoses & Disposition
Evolving Diagnoses
- [S01E01]Ventricular Tachycardia
- [S01E01]Severe Hyperkalemia
- [S01E01]Rhabdomyolysis with Acute Renal Failure
- [S01E01]Uremic Pericarditis resulting in Cardiac Tamponade
Current Disposition
Stabilized in the ED following emergent pericardiocentesis. Awaiting immediate hemodialysis and eventual transfer to ICU.
Casebook Analysis
Episode Context
Otis serves as the high-acuity 'medical mystery' action case that allows the senior attending (Dr. Robinavitch) to showcase his diagnostic brilliance, decisiveness, and procedural skills to the new interns and med students. It establishes the chaotic, high-stakes nature of the ED and the necessity of trusting clinical instincts over waiting for lab confirmations.
Attending's Review
Medical Accuracy
The presentation of rhabdomyolysis causing hyperkalemic cardiac arrest is clinically accurate and a classic emergency medicine scenario. Treating the EKG changes with IV Calcium prior to lab confirmation is standard of care and demonstrates excellent clinical judgment. The use of insulin and glucose to shift potassium is also correct. While a uremic pericardial effusion causing tamponade is a known complication of severe renal failure, its sudden onset immediately following resuscitation in the ED is slightly compressed for dramatic television effect.
Complications & Errors
- The administration of sublingual nitroglycerin at triage before a full evaluation was risky, especially since his symptoms were driven by an electrolyte-induced arrhythmia, not ischemia.
- A fellow doctor hesitates to push Calcium Gluconate without labs due to the theoretical risk of hypercalcemia. Dr. Robby correctly overrides this, emphasizing that in the presence of wide QRS and peaked T waves (EKG evidence of hyperkalemia), withholding calcium is a fatal error.
Clinical Pearls
In a suspected hyperkalemic arrest, treat the EKG. Widened QRS and peaked T-waves warrant immediate IV Calcium Gluconate (or Chloride) to stabilize the cardiac membrane.
Rhabdomyolysis from extreme physical exertion (like a marathon) can cause profound acute kidney injury due to myoglobin toxicity, rapidly leading to life-threatening hyperkalemia.
Cardiac tamponade is a clinical diagnosis strongly supported by POCUS demonstrating a pericardial effusion with diastolic collapse of the right atrium or right ventricle. Removing even a small volume of fluid (e.g., as little as 3-50 cc) can drastically improve hemodynamics by shifting the patient back onto the steep portion of the Starling curve.