History of Present Illness
Patient fell from a subway 'T' platform and her foot was caught between the platform and an incoming train, resulting in a severe degloving injury and open fracture dislocation of the right lower leg and ankle. The mechanism of the fall is initially unknown; bystanders report she may have fainted, tripped, or been pushed. She was rescued by a Good Samaritan who sustained a head injury in the process. Patient presents with extreme pain refractory to initial opiate administration and an inability to provide history due to a profound language barrier.

Emergency Department Course
Trauma Triage and Initial Assessment
Arrival via EMS post-subway platform fall and crush injury.
+1
Trauma Triage and Initial Assessment
Arrival via EMS post-subway platform fall and crush injury.
Medical Decision Making
Primary survey intact (Airway, Breathing, Circulation are perfect). Given the un-witnessed fall, MDM must account for medical causes of syncope (TIA, CVA, arrhythmia) vs. mechanical fall or assault. Extreme pain requires immediate analgesia, but systemic opioids could cloud mental status, confounding the neurological exam for potential occult head trauma.
Diagnostics & Findings
- EKG
- Troponin
- Head CT
- Pan Scan (Trauma Protocol)
Findings:
- Degloving injury to right lower leg
- Open fracture dislocation to the ankle
- No obvious head trauma on primary survey
- Patient awake but screaming in pain, unable to communicate in English
Interventions
- Fentanyl 50mcg IV (administered by EMS/Nurses, ineffective)
- Cefazolin 2g IV
- Gentamicin 400mg IV
⮑ Outcome & Reassessment
Patient continues to scream in severe pain; 50mcg fentanyl provided zero relief. Communication remains impossible due to language barrier.
Clinical Media

Pain Management Intervention
Refractory pain and debate over systemic vs. regional analgesia.
+1
Pain Management Intervention
Refractory pain and debate over systemic vs. regional analgesia.
Medical Decision Making
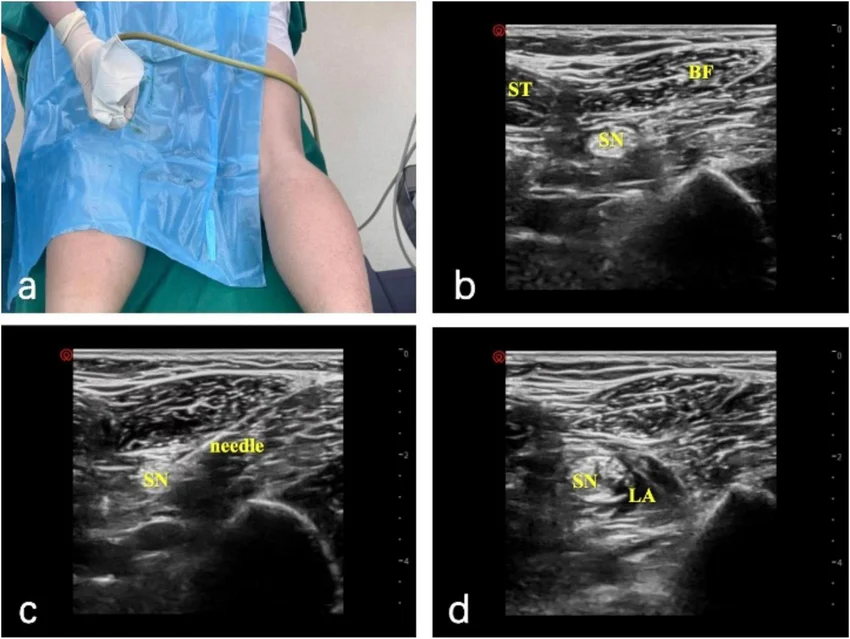
Dr. Collins refuses to push Morphine as requested by Dr. Garcia, citing the risk of clouding the patient's mental status before a definitive neuro exam and Head CT can rule out intracranial pathology. They opt for a regional Popliteal Nerve Block using Marcaine, which will provide localized anesthesia to the lower leg without systemic sedative side effects.
Diagnostics & Findings
Findings:
- Inability to perform thorough physical exam due to patient's extreme pain and thrashing.
Interventions
- Ultrasound-guided Popliteal Nerve Block with Marcaine
⮑ Outcome & Reassessment
Block is completed. Takes ~10 minutes for full effect. Patient begins to calm down, allowing for safer transport to CT.
Clinical Media
Orthopedic Procedure
Requirement to reduce the open fracture dislocation prior to CT scan to prevent further neurovascular compromise.
+2
Orthopedic Procedure
Requirement to reduce the open fracture dislocation prior to CT scan to prevent further neurovascular compromise.
Medical Decision Making
Before reduction, the clinicians must consider the vascular status. A completely transected artery might spasm and thrombose (hemostasis), but a partially cut artery will bleed profusely upon manipulation. They must obtain a deep tissue/bone culture of the exposed fibula prior to reducing the contaminated bone back into the soft tissue envelope.
Diagnostics & Findings
- Wound Culture of open fibula
Findings:
- Grossly deformed ankle with exposed fibula.
Interventions
- Manual reduction of fracture dislocation (Garcia stabilizes knee, Collins distracts distally and moves medially to clear the tibia)
⮑ Outcome & Reassessment
Fracture successfully reduced. The visual severity of the injury and the reduction process causes medical student Victoria Javadi to faint.
Clinical Media


Diagnostic Review and Disposition Planning
Pan scan results return negative for concurrent traumatic injuries.
Diagnostic Review and Disposition Planning
Pan scan results return negative for concurrent traumatic injuries.
Medical Decision Making
With a negative pan scan, the immediate trauma is isolated to the orthopedic injury. Garcia suggests admitting directly to Orthopedics. Langdon counters that the un-witnessed fall (potential syncope) represents an underlying medical etiology that Ortho will not manage. They agree the patient requires a primary Medicine admission for the syncope workup, with Orthopedics following as a consulting service for the leg.
Diagnostics & Findings
- Review of Pan Scan
Findings:
- Negative pan scan (no intracranial hemorrhage, no blunt thoracic or abdominal trauma).
Interventions
- Administration of previously ordered IV Ancef and Gentamicin confirmed
⮑ Outcome & Reassessment
Patient remains stable but disposition is delayed pending Internal Medicine and Orthopedic consults. Language barrier persists.
Social / Language Intervention
Ongoing inability to obtain medical history or consent due to unidentified language.
Social / Language Intervention
Ongoing inability to obtain medical history or consent due to unidentified language.
Medical Decision Making
Previous attempts with language services failed (suspected Pakistani/Urdu/Hindi but incorrect). Dr. Collins uses geographical mapping and pointing to establish the patient's country of origin to request the correct interpreter.
Diagnostics & Findings
- Geographical mapping interview
Findings:
- Patient identifies herself as from Nepal, speaking Nepali.
Interventions
- Requesting Nepali interpreter services
⮑ Outcome & Reassessment
Language identified, enabling proper medical history gathering and informed consent for upcoming orthopedic surgery.
Diagnoses & Disposition
Evolving Diagnoses
- [Trauma Triage]Type III Open Fracture Dislocation to the Ankle with Degloving
- [Diagnostic Review]Syncope of Unknown Etiology
Current Disposition
Admitted to Internal Medicine with Orthopedics consult for surgical management of open fracture.
Casebook Analysis
Episode Context
The patient serves as a high-acuity, visually dramatic trauma case to kick off the episode. Her case establishes the chaotic nature of 'The Pitt', introduces the conflict between the compassionate/cautious resident (Collins) and the skilled but abrasive surgeon (Yolanda Garcia), and acts as the catalyst for the Good Samaritan (Sam Wallace) who ends up with a traumatic brain injury. Furthermore, the gruesome nature of her injury triggers the MS3 (Javadi) to faint, setting up Javadi's character arc of dealing with imposter syndrome and extreme pressure.
Attending's Review
Medical Accuracy
The medical management is highly accurate. Using a Popliteal Nerve Block for a severe lower extremity injury to avoid systemic opioids in a patient who requires a Head CT is excellent, standard-of-care emergency medicine. The administration of immediate broad-spectrum antibiotics (Cefazolin and Gentamicin) for a Type III open fracture is perfectly aligned with ATLS and orthopedic guidelines. The debate over admitting to Medicine vs. Ortho is a very realistic depiction of inter-departmental politics when a surgical patient has an underlying medical issue (syncope).
Complications & Errors
- The initial attempt to push Morphine before clearing the head via CT or establishing a reliable neuro exam could have been an error, though Dr. Heather Collins appropriately caught and prevented it.
- The language barrier caused significant delays in obtaining a history; an earlier use of visual aids or a remote video translation service with a wider array of languages might have expedited care.
Clinical Pearls
In severe trauma with a mechanism suggesting potential head injury or unexplained syncope, prioritize regional anesthesia (like a popliteal block) over systemic opioids to preserve the neurological exam.
Always culture an open fracture before reducing it back into the wound bed to ensure accurate targeted antibiotic therapy for subsequent osteomyelitis.
A negative pan scan clears traumatic injuries but does not explain the cause of an un-witnessed fall. Always work up the underlying medical cause (EKG, Troponin, Head CT) in older adults or cases of unexplained syncope.